It seemed like a routine case, like many other fevers.
A young man in his twenties walked into the outpatient department (OPD) of an Urban Health Centre with a history of ten days of illness with persistent fever, fatigue, and no clear diagnosis. In a setting where dengue, malaria, and viral fevers are far more common, there was nothing immediately striking about his presentation. Yet, something about the case felt incomplete, as if a piece of the puzzle was missing.
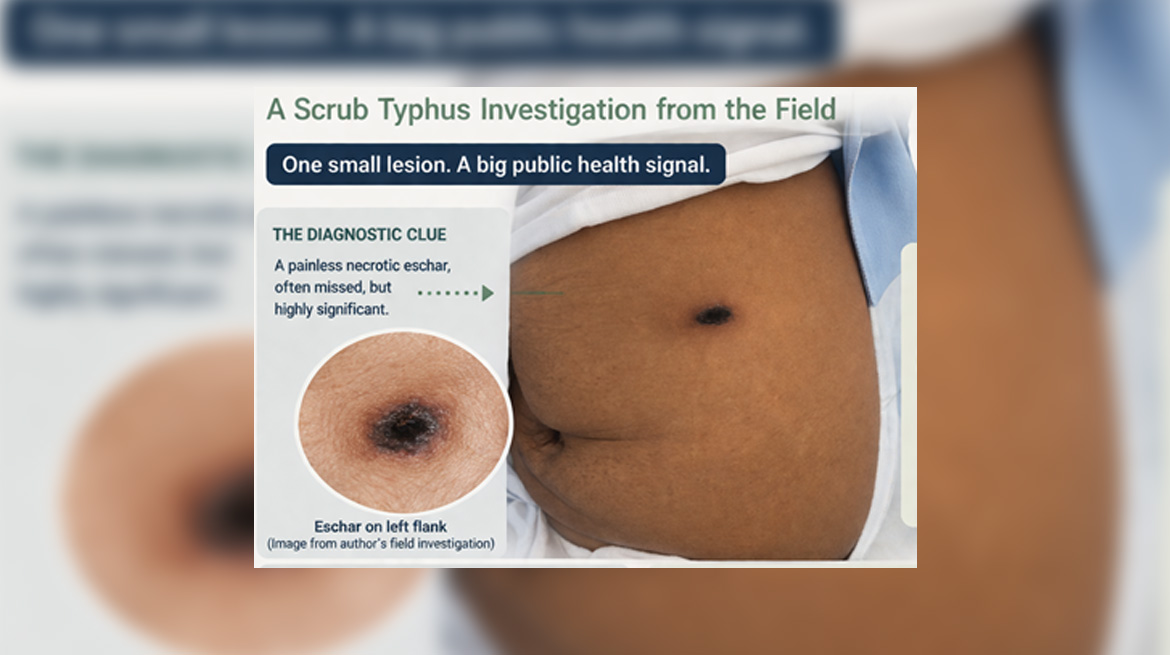
It was not the fever; it was a small, dark lesion over his left flank that caught the attention.
On closer examination, there it was: a necrotic, round eschar on the left flank. A tiny mark, easily missed, yet profoundly significant. That single finding shifted the entire diagnostic direction. Scrub typhus came to the mind as a differential—not as a distant possibility, but as a strong suspicion.
Within 24 hours, serological tests had confirmed the diagnosis of Scrub Typhus.
But the story did not end there.
Beyond the Patient: Asking the Public Health Question
A confirmed case is never just a clinical event—it is a signal.
This patient had no travel history and no exposure to forests or traditionally endemic areas. He lived in an urban setting. If the disease had reached him, it suggested something larger was unfolding.
The question was no longer “What is the diagnosis?”
It became “Where did this come from?”
Into the Field: Tracing the Invisible
The investigation moved beyond hospital walls into the patient’s living environment.
What we found was revealing. During the field investigation, there were multiple rodent burrows in the peri-domestic area, along with poor sanitation and open waste disposal near the kitchen area. Most of the rodent burrows were seen near the open waste disposal site, which allowed easy access to food for the rodents. Another observation was the presence of dense vegetation surrounding the living quarters and the kitchen garden. These were not isolated observations—they formed a pattern.
Soil samples were collected from selected sites around the living quarters and sent for analysis. Laboratory analysis later detected chigger larvae in a proportion of samples, confirming the presence of the vector in the immediate environment.
This was not an imported infection. This was a local transmission.
The Bigger Picture: A Changing Epidemiology
Previously, Scrub typhus has been associated with mostly rural and hilly terrains. However, this case challenges that assumption.
The urban and peri-urban areas are no longer immune.
Rodent–mite–soil interactions, once confined to forests, are now being recreated in densely populated settings—likely driven by unplanned urbanisation, poor waste management, and ecological changes.
The result is concerning; the diseases once considered remote are now quietly emerging within our cities.
The Diagnostic Challenge
Scrub typhus rarely presents straightforwardly.
The presentation often mimics more common febrile illnesses such as malaria, viral fevers, dengue or enteric fever. Symptoms are very nonspecific, and laboratory findings may not be definitive in the early stages. The characteristic eschar, though a pathognomonic sign of scrub typhus, is often missed, especially when located in concealed areas or in individuals with darker skin tones. The eschar is a crucial sign for an early diagnosis, but it is present in approximately half of the patients.
In this case, that small lesion changed everything.
Without an early identification of the lesion, the diagnosis could easily have been delayed, increasing the risk of complications.
The Turning Point: Treatment and Response
As soon as the diagnosis was made, an early treatment was initiated. The patient’s response to treatment was good with doxycycline and became afebrile within 48 hours, with clear clinical improvement.
However, the real intervention extended beyond the individual patient. The real challenge was in the field and at the community level.
Measures were initiated at the community level, including environmental sanitation, rodent control, awareness generation, and strengthening of surveillance. Because in public health, treating one patient is only part of the response—the larger goal is to prevent further transmission.
A Single Case, A Sentinel Event
This investigation reinforces an important principle: one case is not just a case—it is a warning.
The identification of vectors and environmental risk factors in an urban setting suggests the possibility of undetected cases, emerging hotspots, and potential outbreaks.
Ignoring such signals would mean missing a critical opportunity for early intervention.
Lessons from the Field
This experience offers a few important reflections. Not every fever is viral. Clinical suspicion remains one of the most powerful tools in diagnosis. Field epidemiology plays a crucial role and cannot be overlooked. Urban environments are evolving as new risk zones. And sometimes, the smallest clinical clues can uncover much larger public health concerns.
Closing Thought
In medicine, we often search for answers in investigations and reports.
But sometimes, the most important clue is already there—quietly waiting to be noticed.
A small lesion.
A hidden vector.
A much larger story.


